This post is the third in a series on pandemic response planning. See previous posts, Pandemic Emergency Preparedness and Response Planning for Regulated Entities and EH&S Professionals and Pandemic Response Planning: What COVID-19 Is Teaching Us About Risk.
Virtually every preparedness and response plan regardless of the type of emergency it is written for covers three distinct stages: pre-emergency preparedness (prevention/readiness/mitigation), emergency response, and incident termination/resumption of business operations. While there is no required structure or plan organization, we tend to organize preparedness and response plans chronologically according to the three stages while including an upfront emergency response ready-reference guide (we will address this in one of the final posts in this series) that details what needs to happen immediately upon triggering events (e.g., first known human contraction, first human to human transmission, first case in the U.S, etc.).
The pre-emergency components in a pandemic preparedness and response plan should address, at a minimum, the following topics:
- Introduction
- Definitions
- Pandemic Phases
- Pandemic Intervals
- Risk Identification
- Risk Management
- Roles and Responsibilities
- Administrative Controls
- Engineering
- PPE and Emergency Response Equipment
- Drills/Exercises
- Employee Training
- Coordination with Outside Entities
- Business Operations/Continuity Planning
- Communication
- Plan Activation
In this post we provide some key definitions and explain the pandemic phases and intervals. Understanding these foundational concepts is crucial to developing and implementing effective pandemic preparedness and response plans. Moreover, many pandemic preparedness and response plans will include key definitions and describe pandemic phases and intervals in their introduction section. Whether included in a plan or not, the information is helpful as we delve deeper into developing subsequent plan elements in later posts.
PANDEMIC PREPAREDNESS PLANNING INTRODUCTION
Because pandemics are infrequent events, and unless we are pandemic professionals most of us only become knowledgeable about the specifics when we are in the middle of one, it is important to provide basic reference information in the plan as described below.
KEY DEFINITIONS
A complete response plan would likely include additional definitions, some of which would be specific to the organization or facility that the plan covers. For our purposes, we will provide a few definitions that are likely to be included in all plans.
CDC – The Center for Disease Control and Prevention. CDC’s mission is to protect the U.S, from health, safety and security threats by tracking and fighting disease. CDC’s pandemic preparedness efforts include ongoing surveillance of human and animal viruses worldwide, performing risk assessments of viruses with pandemic potential, and developing and improving preparedness tools that can aid public health practitioners in the event of a pandemic.
Epidemic. An epidemic is the rapid spread of disease to a large number of people in a given population/geography within a short period of time.
IRAT – Influenza Risk Assessment Tool. The IRAT is an evaluation tool conceived by CDC and further developed with assistance from global animal and human health experts. It is used to assess the potential pandemic risk posed by viruses that are not currently circulating in people. Input is provided by U.S. government animal and human health experts. Information about the IRAT is available at https://www.cdc.gov/flu/pandemic-resources/monitoring/irat-virus-summaries.html.
Pandemic. A pandemic is an epidemic of disease that has spread across a large region (e.g., multiple continents or worldwide), and is affecting a substantial number of people.
PSAF – Pandemic Severity Assessment Framework. Once a novel virus is identified and is spreading from person-to-person in a sustained manner, public health officials use the Pandemic Severity Assessment Framework (PSAF) to determine the impact of the pandemic, or how “bad” the pandemic could be. There are two main factors that can be used to determine the impact of a pandemic. The first is clinical severity, or how serious is the illness associated with virus. The second factor is transmissibility, or how easily the pandemic virus spreads from person-to-person. These two factors combined are used to guide decisions about which actions CDC recommends at a given time during the pandemic. See https://www.cdc.gov/flu/pandemic-resources/national-strategy/severity-assessment-framework.html.
PPE. Personal Protective Equipment.
WHO – The World Health Organization. The WHO’s primary goal is to direct international health responses within the United Nation’s system. Its main areas of work are health systems, preparedness, surveillance and response on a global level as well as to individual countries and regions that need help.
PANDEMIC PHASES
The WHO pandemic phases depicted below are based on virologic, epidemiologic, and clinical data. The WHO uses the phases to assess and manage risks by identifying and describing evolving situations pertaining to the circulation of novel viruses.
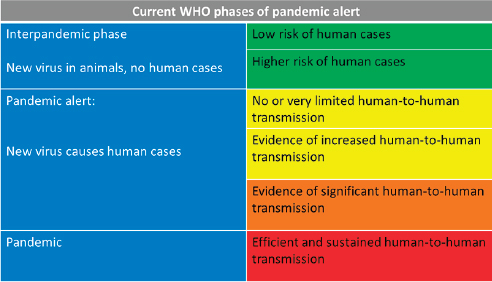
The WHO pandemic phases describe and communicate global disease progression and provide a general view of an emerging epidemiologic situation. The framework for defining each pandemic phase has evolved since the WHO first introduced the concept in 2005. See, CDC report: Updated Preparedness and Response Framework for Influenza Pandemics, MMWR Vol. 63, No. 5 (September 6, 2014). The phases provide specificity for U.S. preparedness and response efforts, and help facilitate initial planning efforts by identifying objectives, actions, policy decisions, and message considerations.
PANDEMIC INTERVALS
The CDC pandemic intervals provide a clearer epidemiologic picture of what is taking place and guide decision makers on when to intervene. See https://www.cdc.gov/flu/pandemic-resources/national-strategy/intervals-framework.html. Epidemic curves are used to monitor an outbreak as it is occurring, describe the outbreak retrospectively, and document the timing of interventions relative to the acceleration and deceleration of the outbreak. For planning and responding to potential pandemics, the CDC describes the six intervals that occur, and which differ by duration and intensity based on many factors (origin location, season of emergence, population dynamics and density, how quickly the virus is detected, success of initial and subsequent containment/isolation efforts, etc.). Like the WHO phases, the CDC intervals are also used to assess and manage risks posed by novel viruses with the capacity to create a pandemic. The image below depicts pandemic phases defined by the CDC.
Preparedness and response framework for novel influenza A virus pandemics: CDC intervals
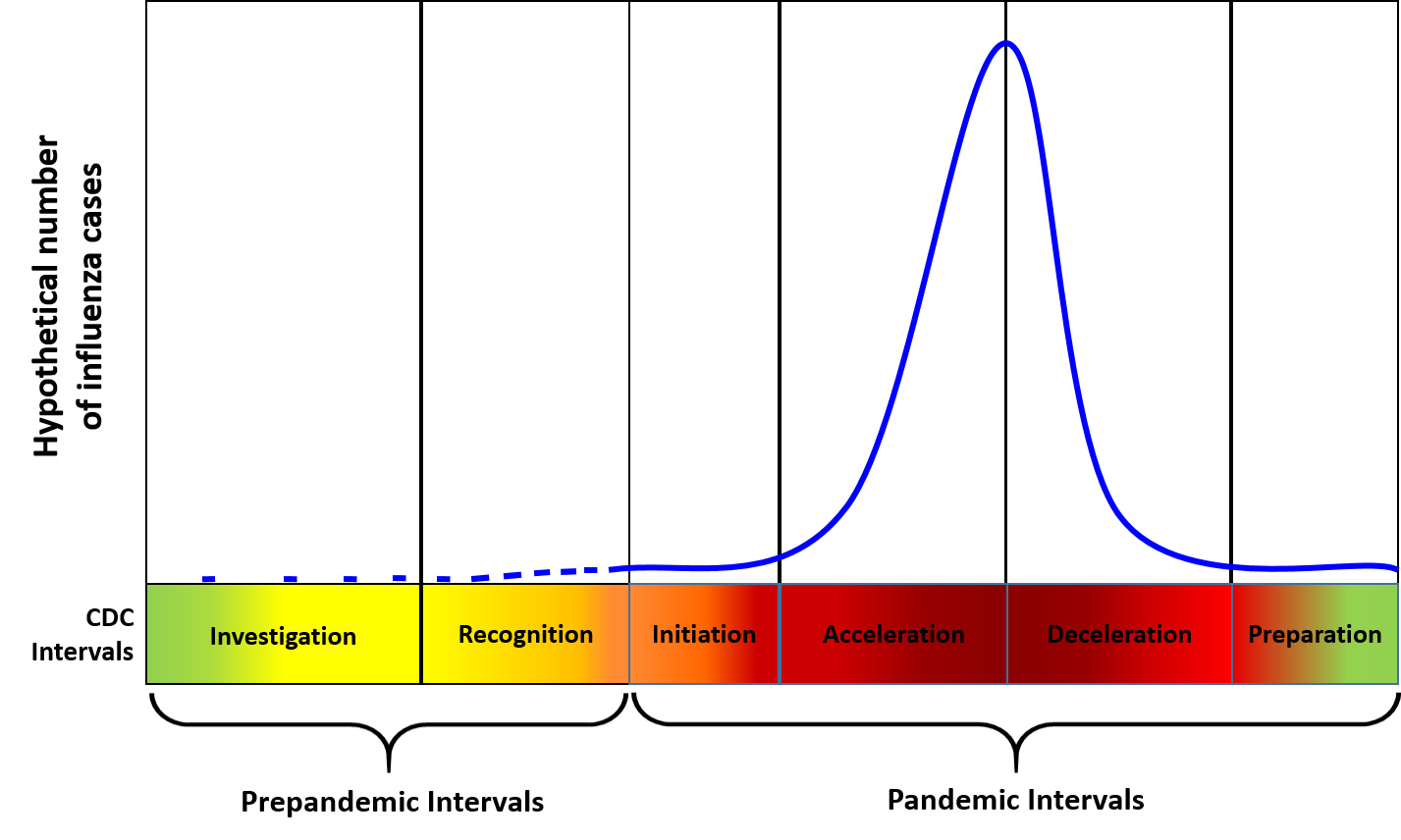
While the intervals were developed for governmental planning, the concepts are also relevant and important to facility pandemic planning and response.
Investigation Interval
The investigation interval is initiated when a novel virus is discovered anywhere in the world and is judged by experts to have the potential to cause severe disease in humans, including person-to-person transmission. Public health actions focus on targeted monitoring and investigation and use of the Influenza Risk Assessment Tool to evaluate if the virus has the potential to cause a pandemic. Co-investigations of animal outbreaks with animal health representatives consider case-based control measures like antiviral treatment, antiviral postexposure prophylaxis of contacts for infected humans, and isolation of humans and animals who are infected. CDC conducts an IRAT assessment during the investigation interval to characterize the potential for emergence, and if the virus does emerge, the severity of human infection. Generally, identification of human cases of a novel virus are reported to the WHO in accordance with the International Health Regulations, although history has taught us that is not always done in a timely and completely transparent manner.
Recognition Interval
The recognition interval is initiated when increasing numbers of human cases or clusters of a novel virus are identified, and the virus’ characteristics show there is increased potential for human to human transmission. Public health actions concentrate on control of the outbreak, with a focus on potential use of case-based control measures, including treatment and isolation of ill persons, and voluntary quarantine of contacts.
As COVID-19 has shown us, some viruses have the potential for extremely rapid human-to-human transmission and global spread. Consequently, facilities should regularly monitor the CDC and WHO websites and begin to activate some of the preparedness sections of their plans (discussed in future posts in this series) once we reach the recognition level. How and when facilities initially act can determine how prepared a facility is to mitigate the risks. For example, NYC hospitals that had on hand or were able to quickly acquire an ample supply of PPE and ventilators in December 2019/January 2020 at the recognition stage, were in a much better position to protect healthcare professionals and treat patients in March than those that weren’t.
Initiation Interval
The initiation interval begins when people are easily infected with a novel virus that can spread in a sustained manner from person-to-person, and human cases are confirmed. Continued implementation of case-based control measures (isolation) and routine personal protective measures (e.g., hand hygiene, social distancing, remote working where possible) is essential, as is enhanced surveillance for detecting additional cases (testing ability and analytical capacity) –which determines when community mitigation measures should be implemented. PSAF results can be used to help ensure that actions are proportional to the severity of the disease caused by the virus.
The initiation interval is the beginning of the pandemic wave and should trigger implementation of the response components of a facility’s (country’s, state’s, city’s) Pandemic Preparedness and Response Plan (discussed in detail in later posts over the next several weeks).
Acceleration Interval
The acceleration interval is when the U.S. is experiencing consistently increasing infection rates and the virus’ epidemiological curve is spiking. Public health actions at this time may focus on the use of appropriate non-pharmaceutical interventions in the community (e.g. school and child-care facility closures, social distancing), as well the use of medications and vaccines if available. These actions in isolation or combined, when available and accessible, can reduce the spread of the disease, and prevent illness or death. Timely implementation of appropriate mitigation measures such as bans on wide-spread mass gatherings, social distancing, the efficient management of public health resources including medical countermeasures and vaccines are of primary importance and may be guided, in part, by PSAF results. Isolation and treatment of ill persons and voluntary quarantine of contacts continue as key mitigation measures. Historical analyses and mathematical modeling indicate that early institution of combined, concurrent community mitigation measures might maximize reduction of disease transmission and subsequent mortality in the affected areas.
Good planning and timely response implementation are crucial to minimize risks from a pandemic. This has certainly played out with COVID-19 to both the positive and negative effect. For example, California and San Francisco in particular acted swiftly in terms of banning professional sports events imposing city and state-wide stay at home orders, school shut-downs, bans on social gatherings and travel and work restrictions; and the population and businesses were very compliant. As a result, what was once seen as one of the country’s hot-spots had, as of April 19 at 9:00 am, limited the number of confirmed positive cases to 1,137 and deaths to 20 (according to https://www.sfdph.org/dph/alerts/coronavirus.asp). In contrast, Florida and Miami in particular did not impose similar mass gathering restrictions or stay at home orders until late March and early April respectively. As of April 19, Miami-Dade County was reporting 10,000 confirmed positive cases and over 200 deaths (According to https://en.wikipedia.org/wiki/2020_coronavirus_pandemic_in_Florida#Statistics).
Deceleration Interval
The deceleration interval occurs when pandemic virus cases decrease consistently in the U.S. Public health actions include continued vaccination (when available), monitoring of pandemic virus circulation and illness, and reducing the use of non-pharmaceutical interventions in the community. During this interval, planning for appropriate suspension of community mitigation measures and recovery begins. State or local health officials might rescind community mitigation measures in certain regions within their jurisdiction. Businesses and facilities begin planning for safe start-up and a return to business as usual or as close to it as the pandemic and the post-pandemic environments allow.
Preparation Interval
When a pandemic has subsided, public health actions include continued monitoring of pandemic activity and preparing for potential additional waves of infection. The preparation interval is characterized by low pandemic activity, although outbreaks might continue to occur in certain jurisdictions. Primary actions focus on discontinuing community mitigation measures; facilitating the recovery of the public health, health-care, and community infrastructure; economic recovery; resuming enhanced surveillance protocols to detect subsequent waves; evaluating the response to the initial wave; and preparing for potential additional waves of infection. Because this interval can last from weeks to months and possibly years, planning and preparation for a subsequent pandemic wave should reflect this variability and cyclical nature until “herd immunity” can be achieved or a vaccine developed. A pandemic is declared ended when evidence indicates that the virus, worldwide, is transitioning to seasonal patterns and gradually taking on the behavior and transmission patterns of seasonal influenza viruses. See https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6306a1.html.
Because pandemics occur infrequently, most facilities’ pandemic preparedness focuses on the first three WHO phases and CDC intervals. The more effort and resources facilities devote to being prepared and equipped to respond to the next pandemic, the lower the negative impacts of the pandemic are likely to be. The next several posts will focus specifically on developing the preparedness components of facility pandemic and response plans.
